A 1984 study proved window views accelerate healing—yet most hospitals ignore this. Discover why evidence-based design loses to cost accounting, and what it costs us.
Hyle Editorial·
A 1984 study found that surgical patients with a window view of trees needed significantly less pain medication and recovered faster than those facing a brick wall. Most hospitals are still built facing the brick wall. The reason is cost accounting, not ignorance.
Roger Ulrich's groundbreaking research at a Pennsylvania hospital tracked 46 gallbladder surgery patients. Those recovering in rooms with nature views required 23% fewer doses of strong analgesics and were discharged nearly a full day earlier. In 2024 dollars, that single day represents roughly $2,800 in savings per patient. Multiply across the 36 million annual hospital admissions in the United States, and the math becomes staggering. Yet hospital administrators continue to approve designs that maximize bed count while minimizing window exposure.
The question isn't whether healthcare architecture affects patient outcomes—the evidence is overwhelming. The question is why we keep building facilities that actively work against healing.
The Science of Sick Buildings
Ulrich's study spawned an entire field: evidence-based design (EBD). In the four decades since, researchers have accumulated a mountain of data showing that hospital architecture directly impacts patient recovery, infection rates, medication requirements, and even mortality.
The Windowless Ward Effect
A 2012 study published in Health Environments Research & Design Journal found that patients in windowless rooms stayed 8.5% longer than those with natural light access. The mechanism is straightforward: daylight regulates circadian rhythms, which in turn regulate immune function, hormone production, and cellular repair. When you remove natural light, you disrupt the body's healing clock.
[!INSIGHT] Hospital windows aren't amenities—they're medical interventions. The American Institute of Architects now recommends a minimum window-to-floor ratio, but compliance remains voluntary in most jurisdictions.
The ICU Noise Nightmare
Intensive care units average 60-65 decibels—comparable to a busy restaurant. Peaks regularly exceed 80 decibels, the level at which sustained exposure damages hearing. For patients trying to heal, this is catastrophic.
A 2017 systematic review in Sleep Medicine Reviews found that ICU patients experience severe sleep fragmentation, averaging just 2 hours of total sleep per 24-hour period. Normal sleep architecture—the cyclical progression through light sleep, deep sleep, and REM—virtually disappears. Without deep sleep, the body cannot release growth hormone essential for tissue repair. Without REM sleep, cognitive recovery stalls.
The result: prolonged ventilator dependence, increased delirium rates, and higher mortality.
“"The acoustic environment in most hospitals is equivalent to a torture chamber for someone who is critically ill. We have known this for thirty years and done almost nothing.”
— Dr. Orfeu Buxton, Penn State University, 2019
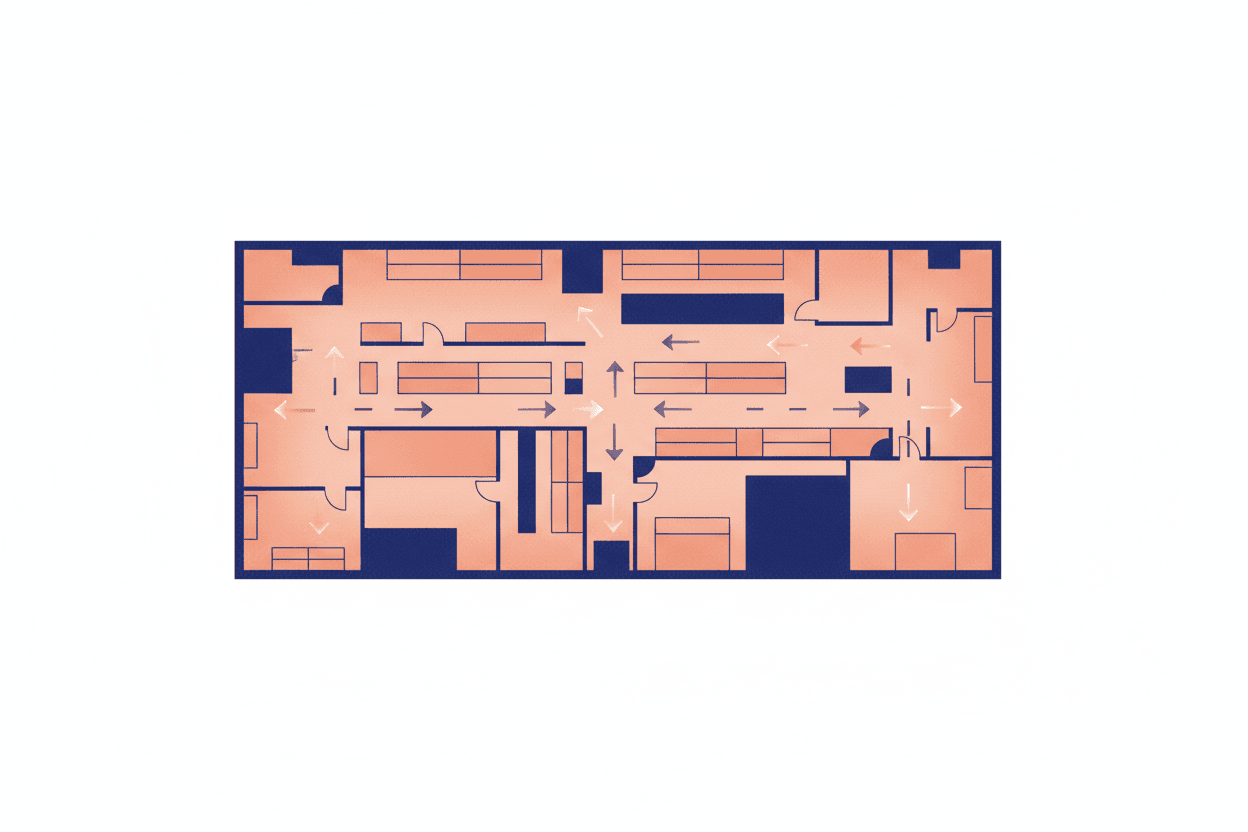
The Labyrinth Effect
Wayfinding—the ability to navigate a space without confusion—is one of the most overlooked factors in patient stress. A 2018 study at a major academic medical center found that patients and visitors experienced elevated cortisol levels when navigating complex hospital layouts. Elevated cortisol suppresses immune function, increases blood pressure, and slows wound healing.
Hospital designers often prioritize staff efficiency over patient experience. The result is a building that makes sense on a flowchart but confuses and stresses the very people it's meant to heal.
The Planetree Alternative
In 1978, a patient named Angelica Thieriot walked out of a San Francisco hospital, horrified by her experience. Cold, impersonal, disorienting—she felt the building itself had made her sicker. She founded Planetree, an organization dedicated to patient-centered hospital design.
Here's where the story gets frustrating. Planetree hospitals don't just feel better—they perform better. A 2020 analysis of 66 Planetree-designated hospitals found:
7% shorter average length of stay
15% lower readmission rates
21% higher patient satisfaction scores
11% lower nurse turnover
[!NOTE] The business case for evidence-based design is well-documented. A 2017 study calculated that a typical 300-bed hospital could save $10 million annually through reduced length of stay alone by implementing EBD principles. Yet fewer than 5% of U.S. hospitals hold Planetree certification.
Why the Brick Wall Persists
If evidence-based design delivers measurable outcomes and clear financial returns, why do most hospitals still look like 1970s office buildings?
The Construction Timeline Trap
Hospital construction projects take 5-10 years from planning to completion. The evidence base for EBD has only matured in the last 15 years. Many hospitals opening today were designed before the research was conclusive.
The Silo Problem
Hospital administrators, architects, and clinicians rarely collaborate effectively. Administrators focus on construction cost per square foot. Architects prioritize aesthetic awards. Clinicians request functional layouts but rarely advocate for healing environments. No single party owns "patient outcome through design."
The Reimbursement Disconnect
U.S. healthcare reimbursement doesn't reward faster healing. Hospitals are paid per procedure or per diagnosis—whether the patient recovers in three days or five. When insurance pays the same regardless of outcome, there's no financial incentive to invest in healing architecture.
[!INSIGHT] Value-based care models—where hospitals are penalized for readmissions and rewarded for quality outcomes—create a business case for EBD. Hospitals in value-based arrangements are 3x more likely to invest in evidence-based design features.
The Path Forward
The next time you walk into a hospital, look around. Notice whether there are windows. Listen to the noise level. Observe whether you feel calm or anxious navigating the space.
These aren't aesthetic preferences—they're health indicators. The building is telling you whether its designers prioritized your healing or their budget.
Key Takeaway: Hospital architecture is a medical intervention. Every design decision—from window placement to acoustic materials—affects patient outcomes. The evidence is clear, the ROI is proven, and the moral imperative is obvious. We know how to build hospitals that heal. We simply choose not to.
Sources: Ulrich, R.S. (1984). "View through a window may influence recovery from surgery." Science, 224(4647), 420-421. | Ulrich, R.S. et al. (2008). "A review of the research literature on evidence-based healthcare design." HERD, 1(3), 61-125. | Xyrichis, A. et al. (2017). "Sleep disruption in the ICU." Sleep Medicine Reviews, 34, 97-107. | Planetree (2020). "Designated Hospital Outcomes Report." | The Center for Health Design (2017). "Business Case for Evidence-Based Design."
This is a Premium Article
Hylē Media members get unlimited access to all premium content. Sign up free — no credit card required.